RSV (Respiratory Syncytial Virus)
 Reviewed by expert pediatric providers
Reviewed by expert pediatric providersWhat is RSV?
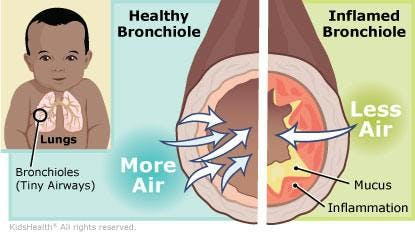
RSV, short for Respiratory Syncytial Virus. RSV can lead to upper or lower respiratory tract illness, and is the leading cause of bronchiolitis (inflammation of the small airways of the lungs). While older children and adults often only appear to have a mild cold, younger children are more likely to have it affect the small airways (bronchioles) in their lungs, which is when it is called bronchiolitis. It typically begins with upper respiratory symptoms of runny nose, nasal congestion, sneezing, and coughing for 2-3 days, and then in younger kids and infants can progress to the lower respiratory tract where it can lead to wheezing and difficulty breathing. Younger children commonly experience fever, though fevers can occur in any age. RSV outbreaks typically occur during the winter and early spring months, but can vary based on the year and in different areas of the country.



Fever (temp of 100.4 or higher)

Runny nose

Nasal congestion

Sneezing

Coughing

Fussiness or irritability

Poor feeding, decreased appetite
Signs that has progressed to lower respiratory tract (bronchiolitis):
- Wheezing
- Faster breathing
- Grunting while breathing
- Nasal flaring with breathing
- Belly breathing (when their belly is moving significantly more than normal with each breath)
- Retractions (if the skin between the ribs, below the ribcage, or in the lower neck above the sternum is sucking inward with each breath)
How severe is RSV?
RSV is not unique to children—adults can get it as well, albeit usually with milder symptoms. It matters for children, especially babies because it’s the most common cause of respiratory-related hospitalization for infants. The overall mortality rate for RSV is less than 1%, and in the United States, there are less than 400 deaths attributed to RSV annually. Most children experience at least one bout of RSV before the age of 2 years.
In infants and children <2 years


Symptoms can vary from fever and cough to development of wheezing and difficulty breathing, to the point of needing hospitalization. Approximately 20% of infants develop RSV-associated wheezing during the first year of life; 2% to 3% require hospitalization. Infants with congenital heart disease, prematurity, chronic lung disease, or those with compromised immune systems tend to be at the highest risk.
In older, healthy, children and adults


Symptoms often mimic that of a common cold, but wheezing can still occur in up to 35% of adults and older children that are affected.
What causes RSV?
RSV is caused by infection from viral particles via contact or inhalation. Close contact with someone who is infected is the most likely source of transmission. It may also be picked up from contaminated surfaces. The virus attaches to and infects cells within the upper and lower airways.
Is RSV contagious?


Those infected with RSV should be considered contagious for 2-7 days on average, but younger children and the immunocompromised can be contagious for up to a month. Adults can infect children and vice versa.
How to protect your child from RSV
What do I do if I think my child has RSV?
Although the symptoms of RSV resemble those of many other common respiratory infections, it can often be diagnosed clinically based on the symptoms your child is experiencing. When necessary, RSV can be identified via several testing methods, most commonly collected via a nasopharyngeal or nasal swab. In some rare situations, a saliva sample or a nasal wash may be used to test for RSV. Along with other vital signs, an oxygen level is typically checked by using a pulse oximeter (a painless device that gently attaches to the finger or toe of the child).
It’s not immediately necessary to distinguish between RSV and other viruses. If symptoms remain mild and the child continues eating, drinking, and passing urine and stool as normal, there is no need for immediate alarm.
However, especially in children under 2 years of age, symptoms may worsen. Concerns over the oxygen levels or pneumonia development due to infection of the lower respiratory tract is something your pediatrician will monitor which may eventually warrant a test for RSV.
Fever above 101

Severe, hacking cough

Discoloration of the skin (bluish) due to lack of oxygen

Secondary ear infections, and croup may develop

For children having difficulty breathing, frequent waking is common, and the child may prefer to sit or lay at an elevated position instead of lying down flat. Infants who are feeding will likely have difficulty, and often appear sleepy and/or irritable.

Wheezing, signs of difficult breathing or retractions, which is when the skin between the ribs or above and below the ribcage gets sucked in when they are breathing.
What to do if your child has RSV
When to seek medical care
Because RSV is a viral infection, antibiotics are not effective in treatment and are not recommended. If RSV is suspected, a clinical evaluation is recommended in order to provide proper diagnosis and treatment. This will result in avoiding overuse of antibiotics, which can result in long-term antibiotic resistance.
Treatment
Most cases of RSV can be cared for at home following a diagnosis with “supportive care.” This could include:
- Managing fevers with over-the-counter (OTC) fever reducers like acetaminophen (Tylenol), or ibuprofen (Advil or Motrin). It is best to dose this according to your child’s weight. You can find Brave Care’s dosing calculator HERE for the most accurate dose.
Note - never give aspirin to children,and ibuprofen is only to be used in children 6 months of age and older. - Plenty of fluids and rest. If your baby is breastfed, offer frequent feedings, and do not supplement with any water. If breastfeeding is difficult for your baby, you can consider feeding expressed breastmilk from a bottle or cup.
- Nasal saline & suctioning: Apply nasal saline spray or drops to nasal passages, let sit for 3-5 minutes. Then using a bulb suction or a Nose Frida, gently suction out mucus from both nostrils. Perform this 3-4 times a day for best results, especially before bedtime and nap, and before eating. (Do not over-suction, as this could lead to increased inflammation in the nasal passages.)
- Use of a cool-mist humidifier at bedtime, naptime, or throughout the day
- Monitoring changes in breathing
- Avoid any smoke exposure to your child
- Do not give cough medicine that contain dextromethorphan to children under the age of 4 due to serious side effects. Use caution even in children 4-11 and always follow package directions carefully.
It’s important to seek medical attention once severe symptoms appear or you notice significant changes in your child’s wellness so that a proper evaluation can be conducted. Most cases are not severe, but distinguishing between RSV and other viruses can help form a better treatment plan.
Duration
Most RSV infections resolve with at-home supportive care in about 1 week. If fever occurs, it generally lasts 2-3 days at most. The worst of the symptoms typically peak around day 3-4, then start to gradually improve. Many children may continue to cough even after recovering. This is commonly referred to as a “post-viral cough,” and could linger for up to 2 weeks, and occasionally longer in some children. After they have fully recovered, the cough should not be treated as a sign of ongoing infection, but for any children with ongoing cough it may be helpful to have them evaluated as a precaution.
How long should my child stay home?
Most people infected with RSV are contagious for 3 to 8 days, though some can remain contagious for longer. There is no way to tell for sure when your child is no longer contagious, but a good rule of thumb is that a child can return to school/daycare once the following criteria are met:
- Fever (temp of 100.4 or higher) is gone for at least 24 hours, without any fever-reducing medications
- They are eating and drinking well
- The cough is not causing significant distress or interfering with talking or normal activity
I’ve heard an inhaler or breathing treatment may be helpful?
For children that have a history of previous recurrent wheezing or asthma (or reactive airway disease, as it is often called when they are younger), albuterol given through an inhaler or nebulizer could be helpful. On the other hand, just because a child is wheezing and is diagnosed with bronchiolitis, it doesn’t mean they need albuterol. In most children with bronchiolitis caused by RSV, albuterol does not provide any benefit.
Anything else?
RSV infection in infancy has been associated with recurrent wheezing and the development of asthma in some patients, though most patients that get RSV do not develop asthma. If your child continues to experience wheezing episodes or frequent coughs, it is important to follow up with your primary care provider.




Dr. Chelsea Roberts was born and raised in the Portland area, and enjoys being able to practice medicine in the community she was raised. After attending Linfield College, she went on to Oregon Health & Sciences University where she received her Masters in Physician Assistant Studies. She then received her Doctor of Medical Science degree at the University of Lynchburg. She is NCCPA certified and has over 13 years of experience as a pediatric medical provider. When not at work, she enjoys traveling, kayaking, camping, and exploring the outdoors with her husband, 2 daughters, and their rambunctious Australian Labradoodle.


